

VITTORIO CAPEZZUTO: FULL DENTURES: A COMPLICATED CASE SOLVED ACCORDING TO THE GERBER CONCEPT – REGAINING CHEWING FUNCTION, FACIAL PROPORTIONS AND DENTO-ORAL ESTHETICS. PART 2 Leave a comment
Fabrication of templates
The functional model was fabricated from synthetic super hard plaster type IV as well as vestibular and lingual silicone masks (Fig. 1). After fabrication of the denture base from cold-curing polymer, the silicone masks were filled with AESTHETIC WAX HARD (CANDULOR). Due to the implants, an impression was taken in the traditional way for the lower model. The bite template was fabricated on the functional model (Fig. 2). In the following clinical visit, the jaw relationship was determined and only in a horizontal plane, as all other references such as the occlusal plane, midline, canine tooth line and smile line were already determined accordingly and correctly beforehand within the context of determining the vertical dimension with the aid of the currently worn dentures (Figs. 3, 4).
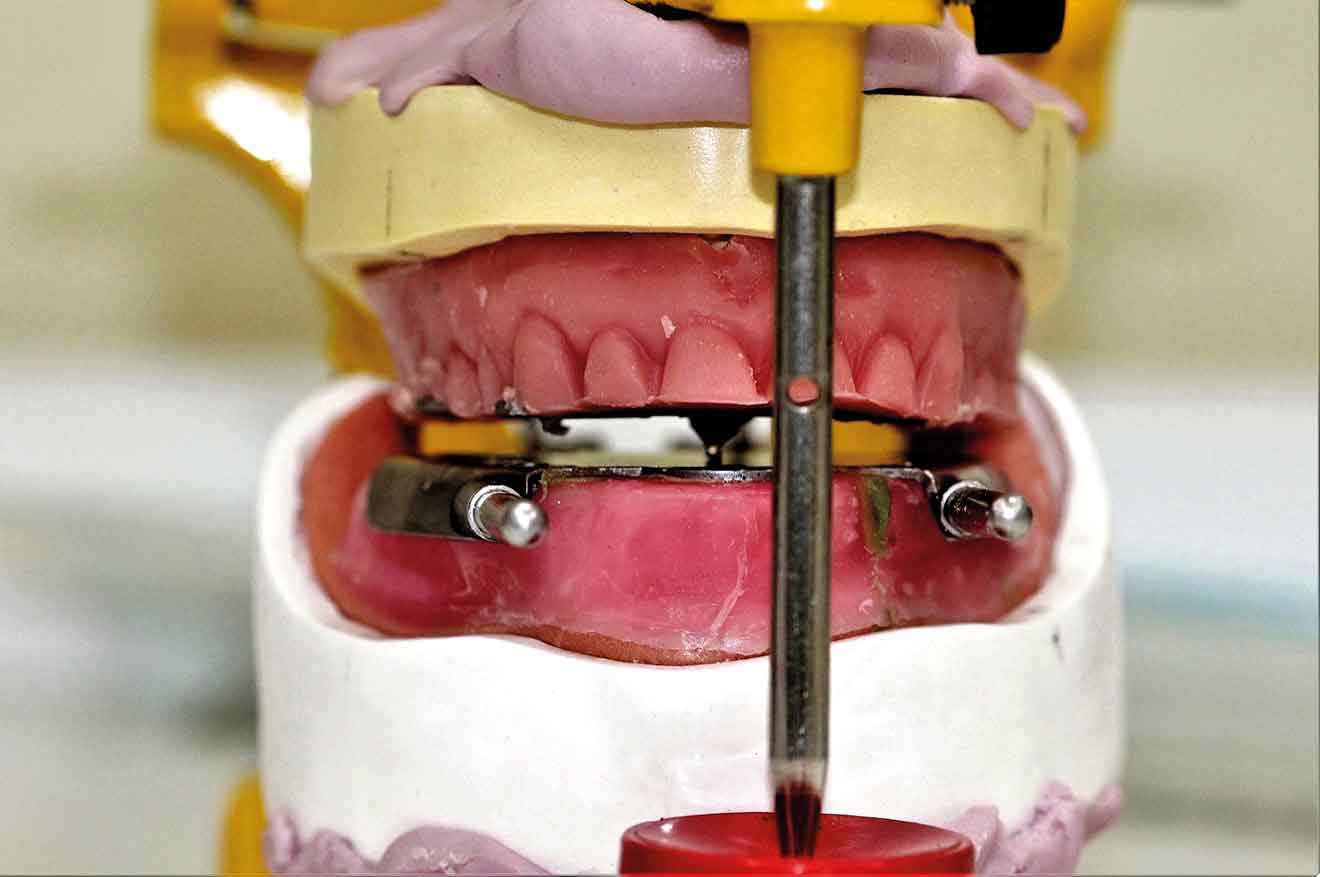
The functional models were oriented at average values in the articulator using a dimensionally stable kneading silicone to be able to fabricate the templates for intraoral support pin registration, which were to be used to record the Gothic arch and to retain the set vertical dimension unchanged for this preparation (Fig. 5). To stabilize the registration pin against vertical forces during registration, the lowest point of the ridge is determined on both sides of the mandibular model and marked on the outer surface of the model (Fig. 6).
The writing plate is mounted in the lower jaw by heating the wax there and pressing it in slightly. Vertical reference is the zero position of the articulator support pin with the upper and lower wax walls lying parallel to each other. Here it must be ensured that both wax walls are harmonized. Then the upper butterfly-shaped plate is mounted to accommodate the registration pin. For this purpose, the metallic registration pin is slightly screwed back so that the tip of the registration pin protrudes, so that its position can already be checked during assembly by the contact point on the lower writing plate.
The plate is also heated for this purpose and carefully pressed onto the upper bite rim. Ideally, the verification contact should be on the line connecting the two lowest points of the lower lateral ridge (Figs. 7, 8, 9, 10, 11).
To allow undisturbed and visually controllable lateral and protrusion movements in the mouth, the upper bite rim is now cut back without changing the vertical dimension of the occlusion (Figs. 12, 13, 14,15).
Support pin registration
In preparation for intraoral support pin registration, the hinge axis points and the outer wall of the joint cusps are determined on the patient so that the facial bow can be anatomically aligned, the sagittal inclination of the joint can be correctly recorded, and correspondence between the hinge axis of the facial bow and that of the articulator can be ensured. For this purpose, two methods have become established to determine the condylar hinge axis at the head: one is statistical, and one is palpatory.
The statistical version states that the condylar hinge axis is located about 13 mm from the line between the temporal eyelid angle and the tragus. For the palpatory method, which we applied here, the patient is asked to perform small mandibular movements to be able to feel the position of the condyle with the small finger in the area of the joint cusp in front of the tragus (Figs. 16). The DYNAMIC FACEBOW according to GERBER (GERBER CONDYLATOR) was used as a face bow with recording of the sagittal joint inclination. This is a kinematic facebow whose correct position is determined by the patient assuming (maximum) retrusion without effort to match the tips with the writing leads with the reference points marked on the skin. Here it is best to follow the “clockwise rule” to check the identification of the hinge axis (Figs. 17, 18).
Sagittal joint path measurement
To record the sagittal joint inclination, the registration cards (Fig. 19) are inserted between the writing lead and the skin so that the lines are parallel to the reference rod of the facial arch (occlusal plane indicator) and thus parallel to the occlusal plane. The patient treated here was asked to perform protrusion movements with her mouth closed. This procedure is repeated three times as a matter of principle to determine the mean value of the sagittal joint path inclination. Here, the so-called “functional” part of the recording is of importance, which corresponds to the probable sliding of the condyles on the joint cusp (tuberculum articulare).
Intraoral support pin registration
This was followed by the intraoral registration of the supporting pin, which was recorded in the horizontal plane (Fig. 20). It is used to determine the horizontal position (sagittal and transversal) of the mandible to the maxilla as “therapeutic” position (Figs. 21, 22). The position is found by comparing the neuro-muscularly determined centric with the vertex of the Gothic arch. Before, the writing plate (lower jaw) is dyed and the patient, like our patient here, is asked to perform eccentric movements – protrusion and laterally to the left and right. The movements mentioned above draw the so-called Gothic arch through the supporting pin (in the upper jaw) onto the writing plate positioned in the lower jaw. The lower registration template is removed, and two lines are drawn on it: the protrusion line and the transversal to the arrowhead. This makes it possible to identify the vertex again and to compare it with the neuromuscular centric. To do this, the surface of the Gothic arch is again dyed before being re-inserted into the mouth. Accordingly, the patient was then asked to perform small opening and closing movements in rapid succession to determine her neuromuscular closing point.
The neuromuscular centric is normally 0.5-1.0 mm anterior to the vertex of the Gothic arch (Fig. 23). If the vertex of the Gothic arch and the neuromuscular centric, as is the case in this patient, are not more than 0.5 mm apart, a Plexiglas disc is fixed to the vertex of the Gothic arch (Figs. 24, 25). If the distance is greater than 0.5 mm, an intermediate position is determined which is referred to as “therapeutic” and lies between the vertex of the Gothic arch and the neuromuscular centric. However, this position must be perceived as being comfortable by the patient. Finally, this position is keyed, in this case with fast setting articulator plaster, which was filled into a syringe for application beforehand (Fig. 26). Once the registration templates are keyed, they are transferred to the articulator (Fig. 27). To transfer the models into the articulator, the writing leads are replaced by metallic reference rods on the GERBER facebow. When positioning their tips in the hinge axis of the articulator, it should be ensured that the metallic reference rods are always parallel to the working plane. During the curing of a low as possible expanding plaster and after removing the wax from the two metal plates (supporting pin and writing plate), the existing silicone keys were used in the upper jaw to restore the part removed for the supporting pin registration and to bring it into contact with the lower wax wall (Figs. 28, 29,30).
Model analysis
The “blueprint” in the form of the model analysis for the wax-up was then prepared in the laboratory. For this purpose, the contour of the alveolar ridge on both sides is transferred to the outer surface of the mandibular model using the profile compass (Figs. 31). The 4 and 6 positions are marked and also transferred to the model outer surface or model margin (Figs. 32, 33). The center of the incisive papilla is determined for the CPC line, the line is extended to the model margin (Figs. 34). This is followed by checking the bilateral ridge profile to determine parallelism or divergence. The stop line is also determined. According to GERBER, in order to avoid forward movement during sagittal frontal and caudal gliding behind this, it is necessary not to set up a masticatory unit in occlusion, any more, which would also lead to premature wear of the retention part in our case due to the implants.
In the next step of the model analysis, it is assessed whether a normal or a cross bite is present, and it is checked whether the alveolar ridge has a distal or a lingual position (Fig. 35). Of course, an experienced eye can detect the situation to be solved in a few minutes and a few work steps in order to recognize how and where anterior and posterior teeth are to be set up. However, it makes sense to record and document as much information as possible. This way, it is possible to make the design of the dental prosthesis more predictable during the set-up phase (Figs. 36, 37) despite the somewhat higher expenditure of time and also to avoid errors.
To be continued next issue…
